Brugada
Syndrome
·
The
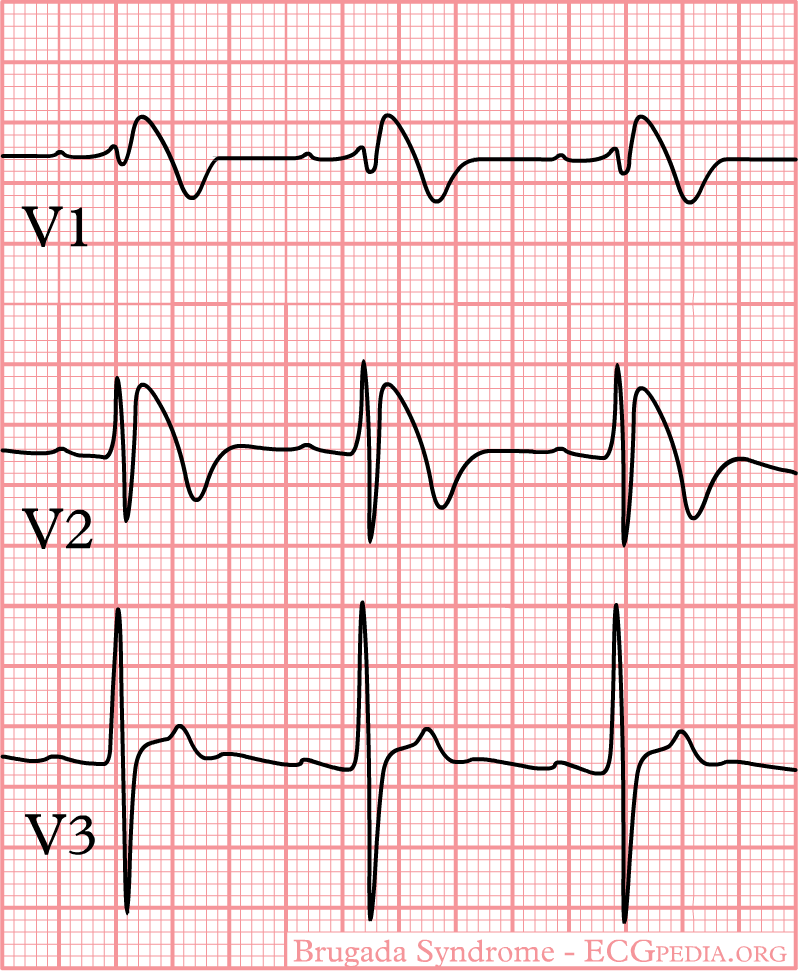
major clinical features of Brugada syndrome include
o manifest, transient, or concealed ST
segment elevation
o in V1 to V3
o that typically can be provoked
with the
§ sodium channel-blocking drugs
·
ajmaline,
·
flecainide, and
·
procainamide and a
o risk
of polymorphic ventricular arrhythmias.
o It appears that a diminished inward sodium current
in the region of the RV
outflow tract epicardium
is responsible for Brugada syndrome (Table 233-8).
o
A
loss of the action potential dome in the RV epicardium due to unopposed ITo potassium outward
current results in dramatic
shortening of the action potential.
o The large potential difference between the normal endocardium and rapidly depolarized RV outflow
epicardium gives rise to ST-segment elevation in V1–V3 in sinus rhythm and predisposes to
local ventricular reentry
(Fig. 233-14).
o The majority of genetic abnormalities
responsible for the syndrome have not been described; however, in ~20% of
patients, mutations of SCN5A
genes have been identified.
o
Although
identified in both genders and all races with an autosomal dominant inheritance pattern, the arrhythmia syndrome is most
common in young
male patients (~75%)
and is thought to be responsible for the sudden and unexpected nocturnal death
syndrome (SUDS) described in Southeast Asian men.
o The ventricular arrhythmia characteristically occurs with rest or during sleep.
Fever and other sodium
channel-blocking drugs have also precipitated ventricular arrhythmias.
·
The
presence of spontaneous
coved-type ST elevation in the right precordial leads and a history of syncope
or aborted sudden cardiac death are predictors of an adverse outcome.
Because of the overlap in SCN5A mutations, the
association of Brugada syndrome with phenotypic LQT3 and conduction
disturbances has been noted.
·
Treatment:
Brugada Syndrome
·
A drug challenge with procainamide may be
important to establish the diagnosis and the probable cause of unexplained syncope when
the surface ECG is equivocal (saddleback ST elevation pattern).
·
Ajmaline
and intravenous flecainide, which are not available in the United States, may
have higher sensitivities for identifying the syndrome.
·
Successful
acute management of recurrent
VT has been reported with isoproterenol or quinidine administration, although experience
has been limited.
·
Patients
who do not benefit from
beta blockers and chronic suppression with quinidine, which may lengthen
epicardial action potential duration by blocking ITO current, may be considered for ICD implantation. ICD treatment to manage
recurrences and prevent sudden death is recommended for all patients who have
had documented arrhythmia episodes and patients with syncope and positive spontaneous
or provoked coved-type ECG ST-segment changes in V1–V3.
·
Family members should undergo ECG
screening for
the presence of the abnormality.
·
The
role of programmed cardiac
stimulation and the use of ICD therapy in asymptomatic patients with the
Brugada-type ECG pattern remain somewhat controversial, as is provocative drug
infusion and programmed stimulation in patients with borderline abnormalities
and no arrhythmia symptoms. Longer-term follow-up in a larger group of these
relatively low-risk patients may be required before definitive recommendations
can be provided. Counseling
on controversies that exist, the potential risk of fever, and inadvertent administration of tricyclic antidepressants
should be considered. Genetic
testing may be helpful in confirming the presence of the genetic
abnormality in family members of patients who manifest the arrhythmia syndrome.
No comments:
Post a Comment